
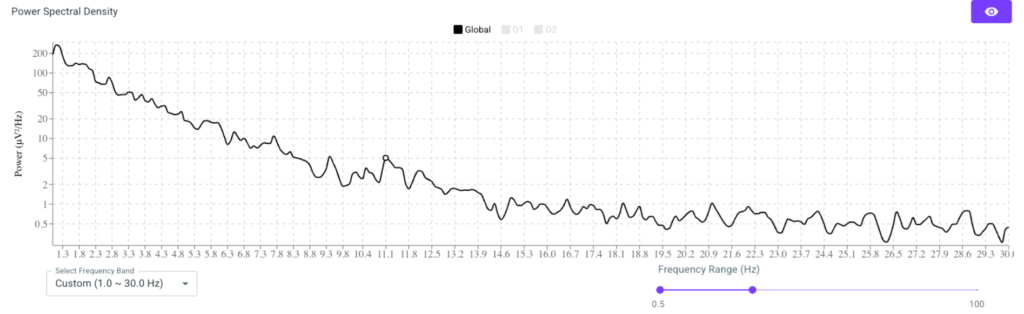
In our latest update, we have enhanced the original Fast Fourier Transform (FFT) chart by implementing a Power Spectral Density (PSD) plot. This modification delivers a more accurate representation of signal power across the EEG frequency spectrum, offering 0.1Hz bin resolution, an improvement over the previous 1Hz bin size. This change is more than technical; it reflects a shift toward clinical precision and alignment to the highest scientific standard.
Beyond FFT: The Case for PSD in Neurofeedback
Traditionally, neurofeedback practitioners have used FFT amplitude charts to visualize brainwave activity. These charts, using 1Hz bins, are helpful for quick reviews but offer limited precision. They average signal amplitude over wide frequency bands and often neglect to normalize power over time or bandwidth.
PSD, in contrast, measures power per unit frequency, typically using methods such as Welch’s averaging technique. PSD offers a higher-resolution, normalized view of frequency content. In our platform, we have moved to 0.1Hz resolution, allowing clinicians to detect subtle shifts such as distinguishing between a peak at 9.3Hz versus 9.8Hz that can influence protocol decisions.
Why 0.1Hz Granularity Matters
Fine spectral resolution enables more than cosmetic improvements. It supports:
- Accurate detection of narrowband features like individual peak Alpha frequencies, SMR peaks, or frontal midline Theta.
- Alignment with neuroscience research, which commonly reports findings using PSD in 0.1Hz steps.
- Improved stability across sessions, as PSD methods segment and average signals to reduce the influence of artifacts.
- Enhanced physiological insight into cognitive function, arousal states, and neuroplastic changes over time.
A 1Hz FFT bin might show general Alpha elevation between 8–12Hz, but a 0.1Hz PSD can reveal a precise peak at, for example, 10.3Hz. This level of specificity enables clinicians to fine-tune protocols with more confidence.
Introducing Peak Alpha Frequency Tracking
Alongside the PSD update, we now offer automated Peak Alpha Frequency (PAF) tracking. PAF refers to the specific frequency within the Alpha band (usually 8–12Hz) where EEG power is maximized. Unlike traditional fixed-band approaches, PAF acknowledges that Alpha peaks vary significantly across individuals and states. This makes it a meaningful, personalized biomarker.
Research consistently links PAF with cognitive performance. Faster PAFs (10.5Hz -12Hz) are associated with superior working memory and processing speed, while slower PAFs (<9Hz) may indicate cognitive slowing, fatigue, or neurological disruption. PAF also fluctuates with factors such as sleep, anxiety, or medication, making it useful for monitoring client state and treatment responsiveness.
Using PSD and PAF in the Divergence System
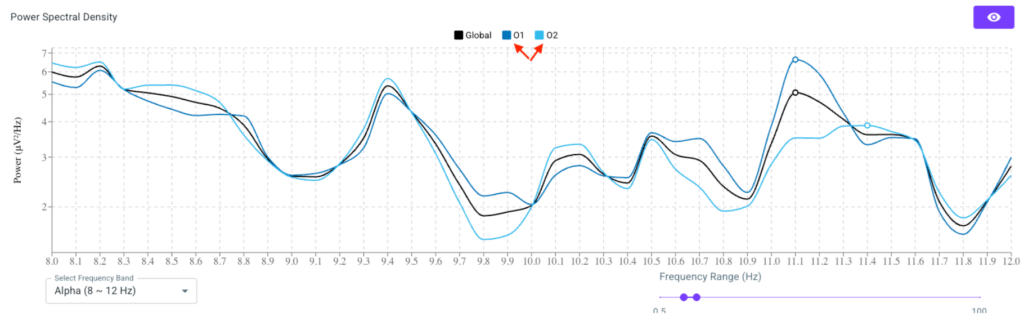
The new PSD graph is accessible in the full spectrum (1.0Hz – 45.0Hz) or within selected bands, such as alpha. Practitioners can explore both global and channel-specific PSD data. By default, the system displays a global average PSD calculated from all channels. Clicking individual channels allows for cross-site comparison and regional analysis.
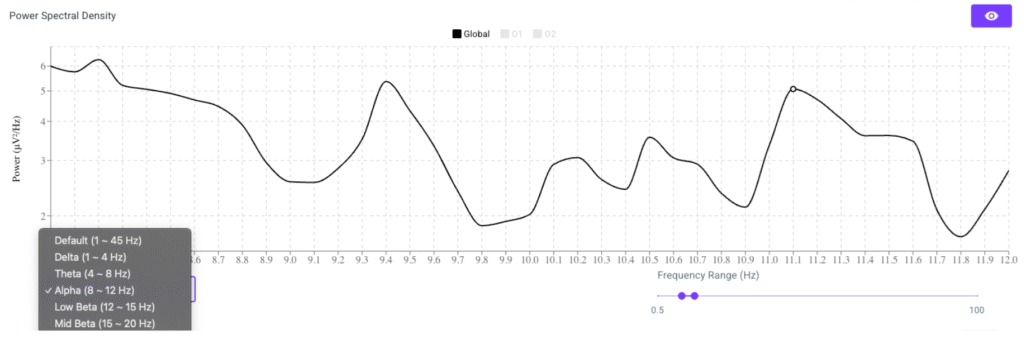
Within the Alpha band view, the system highlights the Peak Alpha Frequency selected by our algorithm. Clinicians can then observe how this peak evolves across sessions in the Session Summary, where we’ve added a dedicated PAF tracking graph. Color-coded markers help distinguish slow, medium, and fast PAF states over time.
This data is now integrated into every biofeedback session record, providing actionable insights with each client interaction.
Why Tracking PAF Supports Better Clinical Outcomes
Practitioners can use PAF data to:
- Tailor neurofeedback protocols around each client’s natural Alpha peak.
- Identify early indicators of cognitive change or emotional stress.
- Monitor recovery from brain injury, aging, or post-viral fatigue.
- Adjust training strategies if regressions or plateaus occur.
- Cross-reference subjective improvements (e.g. better focus or mood) with physiological shifts.
This approach supports a data-informed, adaptive treatment strategy rather than relying on static frequency bands.
Research Supporting PSD and PAF in Clinical Practice
Multiple peer-reviewed studies validate the clinical and scientific value of using PSD and PAF:
- Klimesch (1999): Found that PAF correlates with memory and cognitive processing. Demonstrated that 0.1Hz-resolution PSD is necessary for individual frequency assessment.
- Angelakis et al. (2004): Showed cognitive improvements in elderly participants by targeting neurofeedback training to each person’s true PAF.
- Grandy et al. (2013): Confirmed that PAF is a stable neurophysiological trait across time and age groups, supporting its use for longitudinal tracking.
- Thibault et al. (2016): Advocated for individualized neurofeedback based on spectral markers identified through PSD, not broad-band FFT.
- Barry et al. (2003): Used PSD to characterize EEG phenotypes in ADHD, demonstrating its diagnostic and therapeutic utility.
- López-Sanz et al. (2016): Linked reduced PAF to early cognitive decline, making it a potential marker for neurodegenerative risk.
These findings underscore that modern neurofeedback requires modern tools that offer precision, personalization, and scientific alignment.
Moving Forward
By integrating PSD with 0.1Hz granularity and automated PAF tracking, Divergence Neuro enables clinicians to elevate their practice. These tools offer a more accurate window into brain function, helping to personalize interventions, monitor progress, and validate client outcomes with objective data.
For practitioners focused on delivering high-quality, neuroscience-informed care, this upgrade represents not just a technical improvement but a strategic advancement in how we assess and train the brain.